PROCEDURES
Our medical doctors are highly trained and experienced and are affiliated with the University of Toronto.
They are also on staff and perform surgery at various well respected Toronto institutions, including; St. Joseph’s Health Centre, St. Michael’s Hospital and The Kensington Eye Institute.
A series of reconstructive surgeries are offered for patients who have had previous ocular trauma or complicated ocular surgeries. Depending on the patient's need the following procedures may be offered: 1.) repair of torn or absent iris, termed pupilloplasty 2.) exchange of intraocular lens 3.) repositioning or fixation of dislocated intraocular lens and 4.) repair of damaged cornea. As these surgeries are tailored to the patient's needs, the surgeon will discuss the specifics of the surgery in an individualized manner.
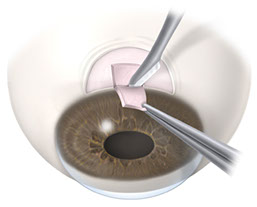
Cataract surgery is performed at either St. Joseph’s Health Centre or Kensington Eye Institute. The procedure is day surgery. Topical drops will be placed on your eye to freeze it. You will receive some sedation through a small intravenous in your hand so that you are relaxed throughout the procedure. During cataract surgery your surgeon will make a small incision in your eye and remove the cloudy natural lens with a special ultrasound, a procedure called phacoemulsification. After removal of the lens, a clear plastic lens called an intraocular implant (IOL) will be placed into the eye to replace the function of your natural lens that has been removed.
What needs to be done to prepare for cataract surgery?
Pre-operative testing
Prior to the surgery you will have an appointment at our office to measure the length of the eye and the shape of the cornea. This will allow your doctor to determine the strength and style of the lens that will give you're the best vision. This measurement will be arranged at the office and can be done with either laser or ultrasound.
Special eye drops will be prescribed for you to take one - three days before your surgery. They will help prepare the eye for surgery. No food is to be taken after midnight the day of surgery. Clear fluids should not be taken 4 hours before your surgery. Regular medications (except diabetic medication) should be taken with a sip of fluid the morning of your surgery. Additional eye drops will be given once you arrive at the hospital.
What Types of implants are available?
The artificial lens implant (IOL) that is implanted into your eye at the time of surgery works in the same way as the natural cataract lens that is removed. The IOL takes the light that comes into your eye through the pupil and focuses it on the retina. The eye relays the light information through your optic nerve to your brain, where the light is analyzed to form images.
Most IOL’s are made of a flexible material and are about one-third the size of a dime. Like your spectacle lenses, your eye will need to be measured to determine the correct power for your IOL, to give you the clearest vision possible.
Intraocular Lens Types
Monofocal Lens
This common intraocular lens provides corrected vision at near, intermediate or far distance. Most people who choose a monofocal lens have the lens set to give them good distance vision and use reading glasses for close activities. Alternatively, a patient may decide to have the lens set so that he/she can read clearly after surgery and then wear glasses for distance. Some patients choose monovision, where one eye is set for distance and the other is set for near. Monovision reduces the need for reading glasses and works particularly well with individuals who use computers or smartphones.
Toric Lens
A Toric lens is a monofocal lens with the addition of astigmatism correction. Patients with astigmatism have a football shaped front surface of the eye instead of being round like a baseball. The abnormal shape causes blurring of the vision both near and far. The toric lens can compensate for the irregular front surface of the eye and reduce the need for glasses post operatively.
Multifocal Lens
Multifocal lenses were developed eliminate the need for any glasses after cataract surgery. Within the implant there are rings that create a series of focal zones that focus light from objects near and far allowing patients both objects.
The ability to read and perform other tasks is variable but is usually best when this type of lens is placed in both eyes. It takes up to 6-12 weeks for the brain to adapt and vision will improve over the first few months after surgery. For many patients these lenses can reduce but not eliminate the need the need for glasses.
Side effects such as glare or halos around lights, or decreased contrast sensitivity may occur. Most people are only mildly affected and the symptoms generally decrease over time. If you are a person that needs good night vision i.e. for driving or if you need very precise close vision, this lens may not be appropriate for you.
What happens after cataract surgery?
After about an hour in the recovery area, patients are usually able to leave the day surgery area, with the assistance of a friend or family member. Most patients will experience some mild eye irritation or discomfort for the first one to two days following surgery, Regular or Extra-Strength Tylenol may be taken.
After your patch is removed, eye drops will be started and will be used for approximately 3-4 weeks after surgery. You will have a follow-up visit with your doctor the same day of surgery or the day after surgery and one week after surgery. A new prescription for glasses will be given 4 weeks after surgery.
What activities are allowed after cataract surgery?
There are few limits on activities after surgery. You can read and watch TV almost right away, although your vision may still be somewhat blurry. Simple tasks such as climbing stairs or walking outside are allowed.
- Avoid eye rubbing or heavy strenuous activity for approximately 2 weeks.
- Avoid getting water in the eye and swimming for 1 week after surgery
What are the benefits of cataract surgery?
Normal or near normal vision may be regained after cataract surgery, if the rest of the eye is healthy. In most cases, it takes the eye approximately 4 weeks to fully heal. Although many patients find much brighter vision and improved colour contrast soon after surgery, it may take several weeks for sharpest vision to return.
What are the risks of cataract surgery?
Cataract surgery is very successful with over 95% of patients having improved vision following surgery, however, as with any surgery, there are risks:
- Infection or bleeding in the eye. This is the most serious risk and also the most rare (1 in 1500) and could lead to loss of vision
- Retinal detachment (1 in 100)
- Glaucoma. This is usually temporary and can be treated with eye drops.
- Need for additional surgery. This occurs when not all of the cataract can be removed safely during the initial surgery (1 in 500)
- Swelling of the retina. This usually occurs weeks or months after surgery and can be treated with eye drops.
When should I call the doctor?
Call the doctor immediately if:
- You have a sudden loss of vision.
- The eye becomes very painful.
- There is a lot of discharge from your eye.
Please go to the Emergency Department if outside regular office hours. Please ask your doctor if there are any further questions.
Collagen cross linking (CXL) is a non-invasive treatment for keratoconus. CXL involves applying a photosensitizing solution consisting of riboflavin (vitamin B2) to the cornea and exposing it to a low dose of ultraviolet light to create new collagen bonds (cross links) throughout the cornea.
In corneas affected by keratoconus, there are too few collagen bonds to maintain structural integrity. The reduced number of collagen bonds and weakened configuration result in corneal bulging, steepening, and irregularity – all of which significantly affect vision.
By creating new collagen bonds, CXL strengthens and adds resilience to corneas weakened by keratoconus. If performed early enough, CXL can counteract the effects of keratoconus and allow good vision to be preserved. In advanced cases, CXL can postpone the need for invasive corneal transplants and prevent vision from getting worse.
Collagen crosslinking is not a cure for keratoconus. The aim of this treatment is to arrest progression of keratoconus, and thereby prevent further deterioration in vision and the need for corneal transplantation. Glasses or contact lenses will still be needed following the cross-linking treatment (although a change in the prescription may be required) but it is hoped that it could limit further deterioration of vision.
Dr.Bujak provides all types of corneal transplants from traditional full thickness transplants named PKP (penetrating keratoplasty) to newer partial thickness transplants such as DSAEK (descemets stripping automated endothelial keratoplasty) and DALK (deep anterior lamellar keratoplasty). Dr.Bujak performs his corneal transplantation at both the Kensington Eye Institute and at St.Michael’s Hospital.
Dr.Bujak is also excited to provide (IEK) Intralase Enabled Keratoplasty. This cutting edge femtosecond laser technology allows the surgeon to precisely tailor the fit of the donor corneal graft to the recipient with precision reaching 5 thousandths of a millimeter.
A cyclodestructive procedure is a type of surgery where a laser light is used to destroy the ciliary body, the part of the eye that produces fluid (aqueous humour). The goal is to decrease the amount of fluid that the eye produces to try to lower the pressure inside the eye. A cyclodestructive laser procedure is usually used to treat severe glaucoma after other forms of therapy have failed. In some specific types of glaucoma it is used instead of other treatments. Sometimes the treatment has to be repeated to get good control of the glaucoma.
Usually this procedure is performed in the Eye Clinic at the hospital. A needle is used to freeze the area around the eye prior to the laser treatment. The procedure itself only takes less than 5 minutes. Your eye will usually be patched after the laser.
Complications of laser cyclophotocoagulation may include:
- Decrease in vision.
- Bleeding from the site.
- Inflammation in the eye (uveitis).
- Pain (may be severe). You will be given a prescription of pain medication at the time of the laser
- Soft eyeball (hypotony), due to a decrease in pressure in the eye. This may lead to clouding of the lens (cataract).
On average laser reduces the intraocular pressure by 30% and most patients can decrease the amount of medications used to control their glaucoma. It is also useful to decrease pain associated with severe glaucoma. Laser cyclodestruction is a safe procedure that can reduce the IOP in the long term in patients with stubborn glaucoma that is not responsive to other therapies.
Intrastromal Corneal Ring Segments (INTACS) is a laser assisted procedure that involves implanting tiny plastic arcs in the cornea. A crescent can be placed in the outer edge of the cornea thus stretching it to make the overall shape flatter.
Since the procedure is used to flatten a steep cornea, Keratoconus patients with steep bulging corneas benefit the most. The advantage of this procedure is that the ring segments can be removed or exchanged. INTACS ring segment implantation is often combined with collagen cross linking and (PTK) phototherapeutic keratectomy.
What is laser Iridotomy?
Laser iridotomy is a laser procedure that makes a small opening in the iris (the coloured part of the eye) to relieve increased eye pressure due to a type of glaucoma called angle-closure glaucoma.
When is it necessary?
A laser iridotomy is necessary as an emergency when a patient is diagnosed with angle closure glaucoma or it can be performed as a preventative treatment in eyes deemed at risk for angle-closure glaucoma.
What is Angle-closure glaucoma?
Angle closure glaucoma occurs when the drainage system of the eye (trabecular meshwork) becomes blocked and the pressure inside the eye increases. The rise in pressure could damage the optic nerve and lead to vision loss.
How do I prevent an angle-closure attack?
An eye at risk for angle-closure glaucoma can be detected as part of a regular eye exam. Using a mirrored lens, your ophthalmologist can determine if the trabecular meshwork is in danger of being blocked.
Risk Factors
People of Asian or Eskimo ancestry have a higher risk of developing angle-closure glaucoma. Increasing age, family history and female gender may also be risk factors.
What are the symptoms of angle-closure glaucoma?
Not all people with angle-closure glaucoma experience an attack. When angle-closure glaucoma develops slowly, there are no obvious symptoms. Symptoms of an attack of angle-closure glaucoma may include: headache or eye pain, blurred vision, halos around lights, a red eye and nausea and vomiting.
What can I expect if I have a laser iridotomy?
The procedure is performed as an out patient in the eye clinic at the hospital. You will be given drops to constrict the pupil and to numb the eye. A special lens will be placed on the eye and the laser will be performed. It takes only a few minutes. It is relatively pain free, however, you may feel a slight pinching sensation.
Following the procedure the vision may be slightly blurred for a few hours, however normal activity can be resumed. You will be prescribed an anti-inflammatory drop to use four times a day for four days after the laser treatment.
Complications
Loss of vision after laser iridotomy is rare. Risks of the procedure include, but are not limited to, bleeding, inflammation and eye pressure elevations. Most of the side effects are mild and temporary.
Phototherapeutic keratectomy (PTK) is a surface ablation corneal laser that assists in removing surface scars and irregularities of the cornea. In select candidates with corneal scarring PTK can be used to improve vision. PTK can also be used to reduce the incidence of painful episodes in patients with recurrent corneal erosions (repeated tearing of the cornea that occurs to patients upon awakening).
Dr.Bujak performs his refractive laser treatments at Herzig Eye Institute. Refractive treatments are designed to decrease a patient’s need for spectacles or contact lenses. Vision correction can be achieved through laser-based methods such as LASIK or PRK (photorefractive keratectomy). Alternatively, vision can be corrected in some patients by implanting intraocular contact lenses such as the Visian ICL. Dr.Bujak tailors the refractive treatment to the patient and their individual needs.
What is Selective Laser Trabeculoplasty?
Selective Laser Trabeculoplasty is a laser treatment that is clinically proven to lower intraocular pressure in patients with glaucoma. SLT can be used alone instead of drops or can be used in patients who are already on treatment when additional therapy is required fro glaucoma control.
How does it work?
The drainage system of the eye is called the trabecular meshwork. The underlying mechanism of SLT is selective photothermolysis. Selective photothermolysis refers to the precise targeting of a structure or tissue using a specific wavelength of laser light. The energy directed into the target area produces sufficient heat to treat the target while allowing the surrounding area to remain relatively untouched. The activated (treated) cells trigger the body’s normal healing response, which helps lower eye pressure.
How is SLT performed?
SLT is an outpatient procedure. During the procedure, the doctor will put anesthetic drops in your eye to numb it, and then place a contact lens on your eye to focus the laser light in the eye. The laser is applied to the trabecular meshwork of the eye. The procedure is generally painless and only takes a few minutes to complete.
Will I feel anything with the laser treatment?
Generally, the laser treatment does not cause pain. However, studies show some patients experience a sensation during treatment. You may see a green flash of light, and feel nothing from the laser. In rare cases, the lens used on your eye may cause some redness or irritation.
What can I expect after the laser?
After the laser you may resume all normal activities. You will be prescribed a topical steroid (anti-inflammatory) drop. The drop is used four times a day for four days after the laser. You will have a follow-up visit after four weeks to check the eye pressure and to determine the effect of the laser.
How successful is it?
SLT is as good as medical therapy for initial treatment of glaucoma. Overall surgeons say you can expect 80% of patients will have good response to SLT. Over time some patients will lose the effect of treatment. However, the laser can be repeated with good results.
A trabeculectomy, i.e., guarded filtration procedure, allows fluid from the anterior chamber of the eye (aqueous) to leak out gradually through a small hole in the wall of the eye (sclera) covered by a thin flap of the patient’s own tissue. The resultant pooling of fluid outside the sclera pushes up the thin, clear, outermost layer of the eye (conjunctiva) is called a bleb. Aqueous leaks from this area into the veins and lymph vessels.
 Trabeculectomy is a surgical procedure to treat glaucoma by relieving high pressure within an eye. It takes the form of a hole covered by a flap (“flap valve”) on the top of the eye hidden under the upper eyelid. It allows fluid within the eye to drain; bypassing the existing natural drainage system of the eye. The flap has stitches in it which can be cut to try to control the rate at which fluid leaves the eye. A trabeculectomy is done in an operating room under local anaesthesia. Usually the procedure takes between 40 minutes to one hour to complete.
Trabeculectomy is a surgical procedure to treat glaucoma by relieving high pressure within an eye. It takes the form of a hole covered by a flap (“flap valve”) on the top of the eye hidden under the upper eyelid. It allows fluid within the eye to drain; bypassing the existing natural drainage system of the eye. The flap has stitches in it which can be cut to try to control the rate at which fluid leaves the eye. A trabeculectomy is done in an operating room under local anaesthesia. Usually the procedure takes between 40 minutes to one hour to complete.
The pressure lowering effect of a trabeculectomy is variable and unpredictable. The body responds to the new drainage hole in the eye in the same way it responds to any cut. It tries to heal it. If the patient creates too much scar tissue, then the flap will seal the drainage hole and the pressure in the eye will rise making necessary a return to drops and possibly a repeat trabeculectomy. If a repeat trabeculectomy is required, the surgeon will usually add a medication such as, 5-FU or mitomycin, to slow down the healing process. If the surgeon feels that the patient may heal too rapidly because they are young, black, have intraocular inflammation, or have had previous eye surgery, then one of these medications is often administered with the first trabeculectomy. Results vary tremendously. However, approximately 50% of trabeculectomy patients will have normal pressures and need no medications for one or more years postoperatively. If medications are added, the success rate of the procedure is over 90%.
Early on after the trabeculectomy there may be an imbalance between fluid made and fluid drained: the new drain may work well, but the eye is not making enough fluid to keep the front part of the eye full and it slowly begins to collapse. At this point, there are several options. If the eye seems to be making a moderate amount of fluid, generally watchful waiting will allow the eye to gradually make more fluid and refill the anterior chamber of the eye. If after several days this does not seem to be happening air or fluid can be injected into the anterior chamber of the eye to refill it. This stimulates the eye into a more normal state of fluid production. If the new drain is working too slowly the pressure in the eye may remain higher than desired. In this case a suture (stitch) can be cut with a laser, to allow more fluid to filter through the new drain to bring the pressure down.
After surgery you may need frequent appointments with your surgeon until the pressure is stabilized. You will need drops to relax the muscle in the eye, to prevent infection, and to decrease inflammation. The results of trabeculectomy surgery vary greatly, and usually depend as much upon the body’s response to the surgery, e.g. inflammation leading to excessive healing or scarring, as it does the surgical technique.
What is laser capsulotomy and when is it necessary?
This procedure is for patients who have had previous cataract surgery and subsequently noticed blurred vision and/or glare and halos around lights.
The natural lens of the eye, is surrounded by a tissue called the capsule. This tissue is left in place during cataract surgery. However, the transparent capsule can opacify over time causing visual symptoms. With the use of a laser, the capsule can be opened up to improve vision.
What can I expect if I have a laser capsulotomy?
The procedure is done in the eye clinic at the hospital using a Neodynium Yag Laser. You will be given eye drops to dilate your pupil and anaesthetize the surface of your eye. A special lens will be placed on the eye and then the laser treatment will be performed. The procedure usually takes a few minutes to complete.
After the laser is completed, you do not need an eye patch. The vision may be slightly blurred for a few hours after. However, normal activity can be resumed.
Complications
In over 98% of yag laser capsulotomy procedures, there are no complications. However, you must be aware in less than 1% of patient’s a retinal detachment may occur. If you notice the onset of flashing lights and/or floaters following the laser treatment; you must call our office immediately for a retinal examination. In less than 1% of patients swelling of the central retina known as cystoid macular edema can occur. This can be treated with drops or an injection and usually resolves but may result in permanent decrease in vision.
Any visual symptoms that are not caused by an opacified capsule such as: retinal problems, glaucoma and/or optic nerve problems won't be improved with the laser procedure. This procedure is covered under OHIP.